
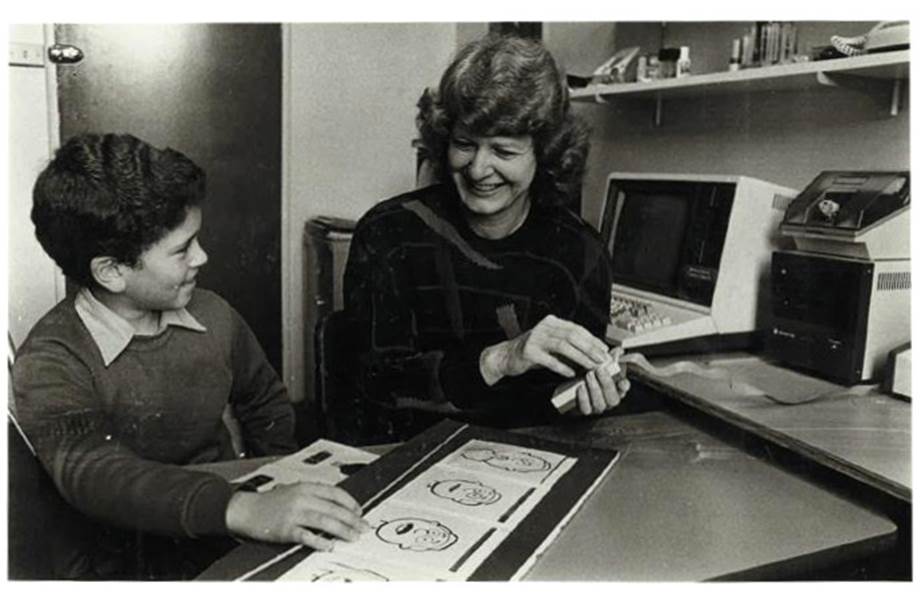
This photo has become an iconic image of the moment an amazing Australian invention changed this young girl’s life forever, and it is known around the world.
Children with cochlear implants: an untold story
4 May 2016
This document is located on the
Suppression of dissent website
in the section on Documents
I had a pioneering role in the field of paediatric cochlear implants in the years between 1985 and 1990, when each step was breaking new ground. I did the initial follow-up work with the first child in the world, Scott Smith, who received a multi-channel cochlear implant from Professor Graeme Clark’s team in Melbourne in 1985. Then, throughout 1986 and 1987, I worked with a group of five children in Sydney with Professor William Gibson. I was responsible for obtaining the pre- and postoperative data on each child, for programming their implants, and for their aural rehabilitation programs.
The work with children captured the imagination of the public as initial results indicated we were witnessing a medical breakthrough. Excitement mounted as news of each child’s surgery broke and it culminated in the live coverage of the “switch-on” for Pia Jeffrey, a congenitally deaf child. Her delightful response to hearing her mother’s voice for the first time was televised live and shown that night on the evening news on every TV channel across Australia.
This photo has become an iconic image of the moment an amazing Australian invention changed this young girl’s life forever, and it is known around the world.
At the end of 1989, after struggling for four years without sufficient funding for the children’s work, I managed to obtain permanent financial support from the New South Wales Health Department that secured the future of the program in the state. However, Professor Gibson became extremely hostile about me doing this. He excluded me from any discussions about how the funding would be used, and took over control of everything to do with it. He then sabotaged me, and forced me out of both the clinical program and the research work. This meant the ground-breaking work I had done with the children could not be published in the scientific literature. It also meant the end of my career.
I went to the Pro-Vice Chancellor’s office at Sydney University to inform them about what happened. About a week later, they contacted me to say they had referred the matter to the Independent Commission Against Corruption because it involved public funds. I had to go to the Commission’s headquarters in Sydney to give a statement, and then served as the key witness in an inquiry that was set up through the university to investigate Professor Gibson’s management of the Ear Foundation.
I have remained silent about these events for the past thirty years because I didn’t want a scandal to damage the work with children. However, I have decided to come forward at this point to provide a factual account of what happened because I recently came across false statements made about my work. I am extremely distressed and angry about these statements, and am writing this article to set the record straight.
More detail about the statements is given in section 13. This is a brief summary.
1. Errors of omission
I am not mentioned by name in any of Professor Gibson’s accounts of the early work in Sydney. My name has been completely erased from the history, and instead, two teachers have been falsely credited with doing the important, ground-breaking research work I did.
2. False and misleading statements about me trying to stop the implant work
In one publication, Professor Gibson falsely implied that I was trying to stop him from increasing the number of implants.
3. False and misleading statements about the Inquiry
Contradictory statements have been made about an inquiry that was held in 1990. One publication implied I was the subject of an investigation because money had been misappropriated. Another publication stated there was an inquiry into my wrongful dismissal. Both these claims are completely untrue.
4. False and misleading statements about the facility
A lot has been made in several publications about one of the neighbours reporting that the rented house for the clinical program was being used as a brothel. I know for sure there were no reports of it being used for this purpose during the year I was running the facility. It may have happened when Professor Gibson took over the management, but this hasn't been stated. This is misleading to readers.
The following sections provide a factual account of the early years of the children’s program in Sydney. I have relied on written notes I kept at the time, as well as copies of the letters I wrote to Professor Gibson and the written report I gave to the Pro-Vice Chancellor’s office about Professor Gibson’s conduct. In addition, there are links to photos, video clips, media articles, and payslips.
I only ever wanted to work with deaf children. It was my calling, ‘mon métier’. I loved it, because “language” fascinates me, and that is what teaching deaf children is all about. Verbal language is such a struggle for them, yet it is at the core of our humanity; it is our birthright.
I first came across cochlear implants in the early 1970s when I had just begun teaching. I went to a presentation by Professor Graeme Clark at an audiology conference where he was talking about the electrical stimulation of the auditory nerve in cats. His vision was to invent a device that would artificially stimulate hearing. This was so impressive, I thought it might be the “blue sky” of the deaf field, despite all the scepticism that surrounded his work. I made a mental note to keep an eye on developments, and then immersed myself in my new role as a teacher.
My next encounter with implants was in 1977 at McGill University in Montreal, when I was doing a master of science degree. My specialty area was aural rehabilitation. A teenage boy with a single-channel device from the House Clinic in Los Angeles came to Montreal, and the head of our program, Professor Daniel Ling, tested his speech discrimination skills in one of our classes. Basically, the boy could tell whether sound was on or off, but nothing else. He couldn’t discriminate been vowels; he couldn’t discriminate between consonants; he couldn’t tell words apart; he couldn't do very much at all. No one at McGill was impressed with what cochlear implants offered at that stage.
Then, in 1978, I returned to Australia to collect the data for my master’s research, and went down to Melbourne with Professor Ling to visit Professor Clark’s program. One adult, Rod Saunders, had an implant at that stage, and we were keen to see what he was able to hear with the device. The team showed us a video of him listening to a newspaper article being read out while turned away from the audiologist. He then turned around and paraphrased the article so well we literally couldn’t believe what we had just witnessed. It was a world apart from what we had seen with the single-channel device.
The possibilities for deaf children were enormous, and I asked Professor Clark when he would be commencing work with this population. It turned out to be several years away because he wanted to establish the implant’s effectiveness with adults first. I asked him if I could join his team when they did start working with children, to which he replied “If you have a PhD”. So I went back to Montreal to complete my masters research and enrol in the doctoral program.
I obtained the highest grade for my thesis in the history of that highly respected research centre. It was a landmark study that was published in its entirety as a book. I could have gained entry into any doctoral program in North America, but chose to stay at McGill because it was the leading centre for aural rehabilitation in the world, and I was involved in all facets of their program: research, clinical work and professional development programs.
I chose a topic for my PhD thesis I thought would be useful for evaluating the effectiveness of multi-channel implants. It was on discourse comprehension. I was interested in the effect a degraded signal might have on our ability to cognitively process and comprehend connected discourse. How well can we make inferences, fill in gaps, predict outcomes, think of analogies, cast judgements and draw conclusions, etc., while we are listening to information, if the speech signal is limited in any way?
At the end of 1983, I contacted Professor Clark again to let him know I was about a year away from completing my doctorate, and he told me they were also about a year away from starting to work with children. So it was all coming together.
I returned to Australia for Christmas 1984, and in the new year went to Melbourne to join Professor Clark’s team. It was an extraordinary year that culminated in the first child in the world, Scott Smith, being implanted. He was a 10-year-old who had lost his hearing after having meningitis in early childhood. He was brilliant to work with and made enormous progress once he had the implant.
I obtained my first insight into how effective this device was going to be with children in the work I did with Scott. It appeared to me that he was able to tap into his auditory memory of the language he had developed prior to losing hearing in early childhood. I found this through the love he had for hearing stories. He would say to me as soon as I picked him up from his classroom for our session together that he wanted to hear a story. Then he would look as if he was in a reverie as he repeated sentence after sentence of the story I was reading out to him. It was a completely different level of language from what he used in normal communication, and it looked as if he was remembering his experience of using language and hearing stories as a young child. It was quite amazing, and I would have loved to have continued working with him. However, I had to move to Sydney at the end of the year because my husband was going to do his doctorate in law at Sydney University.
In January 1986, Professor William Gibson announced he was going to start a pilot program for children with cochlear implants at Sydney University, and he employed me to work on the project with him. We were a team and, as such, were both involved in the selection of the children for the pilot program; Professor Gibson did the surgery, and I did the pre- and post-operative data collection, the programming and the aural rehabilitation programs.

Dr Gaye Nicholls and Professor Gibson with Holly McDonell, Pia Jeffrey, Alison Vary and Joseph Silipo
The programming was a complex process in which I had to work interactively with each child to establish the settings for each electrode on the thin filament that had been inserted inside their cochlear. This was done via a computer that was linked to their speech processor. Each of the 22 electrodes had to be set individually at a comfortable level of loudness, then, all the electrodes were “switched on” so the child could hear speech.
The programming was a process of refinement, and adjustments had to be made over time as the children became more familiar with the speech signal, and more experienced with the process of setting the levels for the electrodes. The objective was to give them the best possible signal right across the speech frequency range, so they could hear everything from the low frequency vowel sounds to the high-frequency, soft sibilant sounds.
I was the only person who did the programming with children during the first four years of the children’s program in Sydney. It was a huge responsibility, and it was as important as the surgery to the outcome for each child. I had to learn everything by doing it myself because there was no one else to watch. However, I had a great deal of support from the people at Cochlear Pty Ltd. Their head office was at Ryde which was only a short distance from where I was based at Chatswood. I was able to talk things over with top experts in the field like Jim Patrick, Chris Daly, Leo Port and Trish Antognelli and get their input at any time. I will always be grateful for their patience, their expertise, and the support and encouragement they gave me in those early years.
The aural rehabilitation work was another matter entirely, and it had no defined end point. It was well-known in the field that early intervention led to the best outcomes for speech and language development, but we were going to be working with older children whose language was delayed. How long it would take them to acquire verbal language with the signal they heard from a cochlear implant, and what the process would be, were unknown. We were in uncharted waters. I was very much looking forward to doing research on this aspect of children’s development as the field of paediatric cochlear implants evolved.

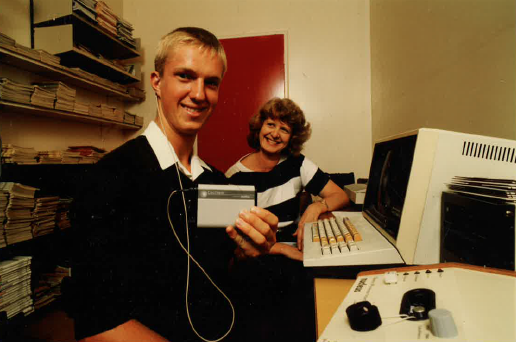
Left to Right: Dr Gaye Nicholls, David Suutari, Pia Jeffrey, Holly McDonell, Wendy McLean, Joseph Silipo
The pilot program started with two teenagers, David Suutari and Wendy McLean, then we worked with Joseph Silipo, a 10 year-old, who had become totally deaf at 3.9 years of age from meningitis, a 5 year-old girl, Holly McDonell, who had become totally deaf from meningitis 8 months previously, and finally Pia Jeffrey who was congenitally deaf.
Working with these children was a journey of discovery that was the most momentous period of my life. It was massively exciting. It was as if the children and I were on a great adventure into the unknown. They put their trust in me and grew in confidence with every step along the way. Yes, there was opposition from colleagues and other professionals in the field, but somehow it was as if the children and I were in a cocoon, cushioned and protected from other people’s scepticism by our own success. I knew, and the children knew, we were onto something special.
David and Wendy mainly benefited from the implant by using it to support lip-reading, which in their case was important. But the three younger children absolutely took off with their new ability to hear. Within 6 weeks of the ‘switch on’, Joseph was able to get 50% on open set sentences through hearing alone, which was simply amazing. He had been totally deaf for 6 years, yet he was able to hear so well, so soon. Holly was following stories through hearing alone within the same amount of time, and she did this without giving the story her full attention. And Pia, well she was right at the beginning of language development, but the benefit to her was just as dramatic in another way. I could say any phoneme I liked to her and she could imitate it through hearing alone. Just imagine that. Here she was, a totally deaf child from birth who could repeat an “s” or “sh” through hearing alone without any teaching intervention.
I had just completed a masters and doctorate in aural rehabilitation where we learned advanced techniques for teaching speech and language to profoundly deaf children, but it looked as if implants were going to render all these teaching techniques unnecessary. The signal from implants appeared to be so good, they could do it all through hearing.
The success we achieved in the pilot program gained the attention of professionals and the public around the world. Results from the Sydney and Melbourne children’s programs were hailed in the media as a medical breakthrough and the floodgates opened to thousands of deaf children. Cochlear implants turned out to be one of the most important medical advances of the 20th Century, and they have revolutionised the field of deafness.
However, there was a very dark, counter-side to the public acclaim and success. Throughout the entire 4-year period I worked with Professor Gibson, my position was extremely precarious because he maintained there was no continuing source of funds to pay me. I was on so-called “soft money”, which meant funds had to be solicited bit by bit, for example through grant applications, donations and bequests. However, this meant I frequently had to work without pay. In 1986 and 1987, while I was working on the pilot program, two schools for hearing-impaired children helped for some of the time: the parents rallied around and did a chocolate drive to keep me going during a particularly long drought, and I worked without pay the remainder of the time.
This situation didn’t improve when the pilot program had been completed and it became a clinical program. I remained on soft money for the next two years when numbers in the program rapidly increased from the initial 5 children to 25.
Professor Gibson was paying me during this period through the university as a senior researcher. However, I wasn't appointed to that position. He said he only had funds to pay me on a monthly basis, which meant he had to activate my pay by writing a letter to re-appoint me every month. However, he frequently failed to do this. Most months I was put in the invidious position of having to go to his office to plead, beg and cajole his secretary into getting him to write the letter for that month. She became very angry and obstructive about doing this, but I wouldn’t have been paid otherwise.
It was an appalling situation that put me under a lot of stress, and it also put the parents and children in the program under a lot of stress. I was the only person doing the programming and aural rehabilitation at that point, but my position wasn’t secure, and the parents were never sure whether the follow-up work with their children would continue. This obviously heightened their anxiety when they were already dealing with a highly stressful situation. They were taking an enormous risk letting their children have surgery to insert an electronic device inside their inner ear that had not yet been proven to be effective with this population. They were the pioneers and they needed assurance and support, not insecurity and heightened anxiety.
The troubling mess with my pay was exacerbated by the fact that we did not have an appropriate facility in which to work. During the first 3 years, I worked in the book storeroom at the top of a stairwell at Chatswood Infants School. It was approximately 3 metres wide and 4 metres long with barely enough room in which to turn around. This tiny space became quite unworkable when the pilot program was completed, and it became a clinical program. The number of implantees rapidly increased to 25 and there was nowhere to work with them.

Left to Right: George Silipo, Joseph Silipo, Gaye Nicholls, Maria Silipo, Viktorija McDonell, Holly McDonell in the book storeroom at Chatswood Infants School, where I did the programming and follow-up work with the children.
I frequently discussed these problems with Professor Gibson and proposed ways in which we could establish the program on a secure basis, but for the first two years he did nothing. So I began to write to him about my concerns. In a letter I wrote in May 1988, I was literally begging him to apply for government funding to support the project:
“I have enclosed an article about the government funded Cochlear Implant Clinic at the Royal Victorian Eye and Ear Hospital in Melbourne. The government has provided money for implants as well as salaries and administrative costs. Could we please approach Peter Collins for funding for an implant clinic … Could we please try for this?”
Later that year, in October 1988, I wrote:
“I am extremely concerned about the future of the Children’s Project. We neither have salaries in place for the staff, nor a proper facility in which to work. My own salary is only guaranteed until the end of December, and there are no alternative funds in place for its continuation after that date. Although I have worked without a salary for several periods in the past, I am extremely loath to be put in that position again. ... The current group of implantees is not getting a fair deal, and we certainly can’t accept more candidates until the problems are sorted out. However, I do not think the project should be limited by the resources that are currently available. We should be expanding those resources and building a strong program for the children in NSW.”
Finally, after I wrote this letter, Professor Gibson did come up with funds to cover (1) the salary for an assistant to work with the pre-schoolers, and (2) the rent for a house in Chatswood he obtained for the clinical program. On my recommendation, he hired Rosalie Yaremko, who was a master’s graduate from the same postgraduate program in Montreal where I had gained my doctorate. But he maintained he still couldn’t find a way to permanently fund my position, even though the soft-money debacle had persisted for nearly 3 years at that stage. It begs the question as to why he was able to fund my assistant and pay the rent for a house, but was not able to fund my position. I was the person who responsible for this important aspect of the work with children, yet it seemed to me that I was deliberately being kept in an insecure position.
Gaye working with Joseph in the storeroom
During these years, the focus of attention shifted from the surgery to my area of the work. Initially, the announcement of each child’s operation created a lot of excitement in the press, but after the first few had been done, people were more interested in how well the children could hear with the device.
Indeed, everything went “ballistic” after I attended the International Audiology Conference in Jerusalem in 1988, where I showed videotapes of the children in the pilot program. This presentation attracted hundreds of delegates, and you could literally hear a pin drop when they watched as Pia repeated soft sibilant sounds with complete ease through hearing alone. After that, people all around the world were contacting me with requests to visit the program or see videotapes of the children. It was ground-breaking work, and everyone wanted to find out what was happening.
It was bizarre to be receiving so much attention and acclaim from within Australia and overseas on the one hand, yet Professor Gibson was maintaining he still could not come up with a salary to pay me.
This insecure situation was compounded in October 1988 when my husband and I were notified we were getting a baby from Korea through overseas adoption. I wanted to be able to work part-time on postdoctoral research after we picked her up the following March, and needed to have my salary confirmed so we could hire someone else to take over the clinical work I was doing at that stage.
And there was another personal factor that put me in a complete dilemma. My sister had been diagnosed in 1981 with kidney failure when she was 35 years of age. By mid 1989, she was in a critical situation. She had been on dialysis and had had two kidney transplants from cadavers that failed, and was desperately in need of another transplant. A kidney from a live donor was her only chance at that point, and I wanted to give her mine. It was early days for live donor transplants but we had been evaluated as being 98% compatible and I wanted to go ahead. However, I needed to be able to take time off work for a couple of months so I could recover properly from an operation that was more complicated for the donor than for the recipient. Hence my urgent and pressing need to get the funding for a replacement to work with the children who were in my care. It was an absolute dilemma. I couldn’t just leave the children without any programming or follow-up, and I couldn’t bear to watch as my sister’s condition deteriorated further.
I discussed the problems with the program, and my own personal situation, many times with Professor Gibson and tried to impress upon him the dire and urgent need for funding, but my concerns went unheeded. He didn’t organise any support for me in the months leading up to our trip to Korea to pick up our baby. When we returned, I had no alternative but to continue working full-time as a new mother with a 6-month old baby, but it was a totally unworkable situation. There were 25 children in the clinical program and they couldn’t all be followed-up adequately; I couldn’t get an assistant or a replacement to cover for me because there was no funding in place to pay anyone; I wasn’t being paid properly; and, I needed to take an extended period of time off work so I could help my sister who was dying.

Me and my daughter around the time when I made the funding applications
Fortunately, in mid 1989, there was a turning point. The children in 10 implant centres around the world were independently evaluated by Professor Richard Tyler from the University of Iowa. Results from the Sydney group were so outstanding they were clearly in a league of their own.
After these results came out, I decided to take matters into my own hands to secure funding for the clinical program. I wrote four letters in which I outlined the success, and the needs, of the Sydney project, and I pointed out the potential benefit this medical breakthrough offered to thousands of deaf children around the world. The letters went to (1) the NSW Minister for Health, (2) the head of services for hearing-impaired children in the NSW Education Department, (3) the head of the National Acoustic Laboratories, and (4) a private philanthropist, Paul Trainor, who was the former owner of Nucleus Ltd, the company that manufactured the device.
The response was overwhelming, and it was immediate. Professor Gibson called me a couple of weeks after I wrote the letters to say the Minister for Health, Peter Collins had written to inform him we would be receiving an enhancement grant of $377,000 per annum for the clinical program. This funding was for salaries for a multi-disciplinary team of people, and for equipment. As you can imagine, I was thrilled and extremely relieved that finally there would be more clinicians to work with the increasing number of children in the program.
However, Professor Gibson’s reaction was quite different. He was dumbfounded about how this had happened. I told him I had written the four letters, and he was absolutely stunned. He didn’t know what to say, and feigned pleasure at first. We went out and celebrated the occasion by having dinner with about 12 colleagues and parents, and it was a very happy night, but he soon privately let me know his true feelings. He was far from pleased. In fact he was extremely hostile about it, and started admonishing me for having obtained the funding because it supposedly wasn’t my place to do this. From then on, he treated me as if I were a naughty child, and excluded me from any discussions about how the money would be used.
I thought this behaviour was unwarranted as I knew I had every right to apply for grants and obtain public funding for the work I was doing. I wrote in a document I tabled in a meeting on 4 September 1989,
“To be excluded from its [the enhancement grant’s] management is quite ironic when you consider how much the Children’s Project struggled during the time in which we didn’t have adequate funding, how difficult it was to get Bill to think about applying for funds himself, and how desperate I was when I wrote the letters that finally secured the funds.”
Over the next couple of weeks, I personally received responses from the letters I’d written to the NSW Education Department, the National Acoustic Laboratory, and the private philanthropist. They were all extremely positive, and wanted to assist with offers of both financial and “in-kind” support.
1. The National Acoustic Laboratory committed funds for a paediatric audiologist from the organisation to work part time with me to learn the programming procedures and to help ascertain the resource allocations they would provide in the future;
2. The private philanthropist, Paul Trainor, provided an endowment of $100,000 to cover my salary as well as additional funds for the project; and,
3. The Education Department made a commitment to establish an aural rehabilitation unit comprised of two experienced teachers who would provide in-service programs on auditory development to teachers throughout NSW. They also decided to employ a teacher full time to liaise between the clinical program and Education Department teachers.
This was an amazing breakthrough because the head of services for hearing-impaired children, Dr Loretta Giorcelli, had been an arch opponent of cochlear implants throughout the early years. Now she was a firm supporter.
David and Gaye in the storeroom
On 4 September 1989, I called for a meeting with everyone who worked on the children’s implant program. I also requested that Jim Patrick from Cochlear Pty Ltd attend. I thought that with other people present, Professor Gibson might act in a less hostile manner toward me.
I was becoming increasingly alarmed about what I was hearing of Professor Gibson’s plans for the money. He was saying that a large proportion of it would fund 10 implants for child implantees, but I hadn’t asked for this. I also heard he was intending to use part of the money to fund the position for an engineer to work in the 2UE Hearing Centre, and again, I hadn’t asked for this. And finally, Dr Chris Game, an electro-physiologist on the team, told me he had been asked to draw up a proposal about how he could use the funds. All of this meant there would be very little left for the programming and aural rehabilitation work with the children.
In the meeting on 4 September,
(1) I tabled in writing what the funding was meant to be used for (as per the original letters I had written).
(2) I proposed that we engage a management consultant to work with the whole team to develop a management structure and operational systems and procedures for the expanded clinical program; and,
(3) I informed everyone about my urgent need (1) to have an extended period of time off in the short term, and (2) my interest in working part-time in the longer term.
At the meeting, a decision was made that I should inform the parents about all the new developments and a date was set for three week’s time. However, I became aware of various rumblings between Professor Gibson and the parents as the days progressed, and wondered what was going on. I soon found out.
When I arrived at the parents meeting, I was greeted by Professor Gibson and ushered into a room where all the parents were already sitting and waiting. I opened the meeting and started to outline what I was going to cover, but was interrupted by two of the parents who said they didn’t want to hear what I had to say. Instead, they went ahead and read prepared statements condemning me for supposedly withdrawing services. This was bizarre given the fact I had secured a large amount of funding and “in-kind” support to increase the services. However, they wouldn’t let me talk. Then others joined in and it became a feeding frenzy. Obviously, Professor Gibson knew I wasn’t withdrawing services because of the meetings we had had in the lead-up to the parents’ meeting, but he didn’t intervene in any way to stop the madness, or allay their fears.
After he told the parents they should take a vote, I started to think the whole thing might have been set up by him. He asked each of the 40 attendees in turn if they wanted me to continue, and they all solemnly said “no”. I assumed they had either been misled about the new developments and were acting out of fear, or they had been offered some form of enticement to vote unanimously against me.
I left the meeting in a state of shock and despair. However, my position was about to get much worse. I put forward a proposal to Professor Gibson that I step aside from the clinical program and write up the case studies of the children in the pilot program. He agreed to this at first because the parents of the children in the pilot program had signed consent forms for their children to participate in a clinical research study. We were ethically obliged to fulfil our commitment to them to publish the results. I also thought that writing up the case studies was an ideal way for me to continue working in a professional capacity when I had a young baby.
Professor Gibson wrote to the parents saying:
“Gaye is going to spend the next few months publishing this experience and I know she would appreciate your help.”
However, he then changed his mind and told me he wouldn’t let me have access to the files I kept at Chatswood on the children’s pre- and post-operative results, their programming and the aural rehabilitation work. Taking control over these records was unethical. If you think about the situation in reverse you will see how wrong this action was. Just imagine if I had taken over the files Professor Gibson kept at the university on the children’s surgery.
Not only was this action wrong, but it also had serious ramifications because it meant the case studies of the children in the pilot program could not be written, and their story would never become part of the history of this new field.
Then Professor Gibson told me he was making my position redundant.
It was incredible. I was the most experienced person in the field, I had achieved the best results worldwide, I had the highest level of qualifications in aural rehabilitation in Australia, I was a highly respected teacher and clinician, I was an excellent researcher, and most importantly I had obtained permanent funding that secured the future of the program, yet I was being made redundant.
I knew what Professor Gibson had done was unethical, and began industrial action against him for wrongful dismissal. I would have won, because the person who was dealing with the case, Dr Yu (who was the CEO of the Children's Hospital), wanted me to be reinstated. However, Professor Gibson had already written to the parents saying I had resigned from the program, which was completely untrue at this point.
I dropped the industrial action because I realised there was no point in fighting to be reinstated to work with someone who had sabotaged me, and would no doubt only continue to try to damage me. This was an abusive and exploitative professional relationship, and the only thing I could think to do was to get out of it.
Ironically, in a final twist to the pay debacle, I ended up putting my resignation in to the wrong body. After I obtained the funding from the Health Department, Professor Gibson told me my salary was going to be covered by Health, instead of the university. However, I later found out that he didn’t ever make the transfer and I was still being paid by the university on a month by month basis when I resigned. I put my resignation into the Health Department rather than the university, so technically my resignation was not valid. I was just forced out.
I did pursue legal action against Professor Gibson for having defamed me to the parents, and he settled the case rather than face a court of law.
I was sick at heart about having to resign, and could barely function. A couple of weeks later, I was having coffee in the Student’s Union at Sydney University when Lyndall Evatt, the Administrative Officer from Professor Gibson’s office, walked in. She stopped and asked how I was going as she knew what he had done to me. She commiserated about the crazy mess with my pay and said I must have been relieved when the “donation” came in. To which I replied, “What donation?”
Lyndall knew about a large donation Professor Gibson had received from a member of the public who wanted to assist two children, a brother and sister, who had Usher Syndrome. They had been born deaf and were progressively going blind. The donor specifically stated the money was to be used for their follow-up, because he wanted them to be given every possible chance of learning how to use the implant before they became totally blind.
I was stunned, because Professor Gibson had not told me anything about this. I wanted to see if the parents knew anything about the donation so Lyndall and I drove out to their home on the outskirts of Sydney to see them. It turned out that they did know about the donation but Professor Gibson had told them it was to be used for the implants. This didn’t made sense because these parents had already raised the money for their children’s implants through a community fundraising campaign.
I felt sick at the thought that Professor Gibson may have withheld telling me about the donation because it was meant to come to me, which prompted a million questions. Was he really denying these two deaf-blind children the benefit of this donation? Was this money he could have used to make my position secure? Was he going to use it for some other purpose in the implant program that was unrelated to the follow-up work?
I went to the Pro-Vice Chancellor’s office to tell them about my concerns, and they said they would investigate the situation and get back to me. They asked me to write a report about what had happened and they wanted me to include absolutely everything I could think of about Professor Gibson’s character, his behaviour and his management practices. They wanted to get a full picture of what had caused so much damage in this world-leading, high profile project that was a source of pride to the university and to the nation.
The university called me about a week later to say they had referred the matter to the Independent Commission Against Corruption (ICAC). This was unbelievable, and I was both shocked and relieved. I was shocked because it graphically revealed the seriousness of the situation, and I was relieved because it meant all the ethical, management and financial issues I had been struggling with would now be put under intense scrutiny.
When I went to ICAC to give my statement, the investigator explained how their system worked. They only carried out investigations into large-scale systemic corruption themselves. In isolated situations like this, the public body itself had to carry out the investigation under ICAC’s supervision. This way, the organisation would learn how to identify loopholes in its own internal systems and work out ways to remedy any problems. It was an educative process that would put a regulatory framework in place to prevent further corruption from occurring in future. It wasn’t meant to lead to Professor Gibson's dismissal, unless of course there were findings of criminal activity.
The inquiry into the EAR Foundation lasted four months which was a huge undertaking for the panel of academics who were appointed to run it. I was the chief witness, which was extremely arduous, but after I had given my testimony I left knowing I had done everything I could to ensure the children's program would no longer be hampered by the difficult problems I had had to deal with over the first four years. The enhancement grant from the Health Department funding meant the children’s work was now financially secure, and the inquiry into the EAR Foundation meant the research side would be properly regulated.
I then went into free fall. It was like stepping into a void. I was in so much shock and despair, I didn’t know what to think, or how to feel. I was absolutely devastated by the injustice and the unfairness of it all. Not only had the head of the department failed to support me with even the basic requirements of a salary, equipment and a place to work, he had actively undermined me the whole time. After 11 years of university, and the potential to make a significant ongoing contribution to the field, it had all come to nothing.
The hardest thing for me personally was the sudden break from the children in the pilot program. It was as if they had died. I had lived and breathed every moment of their journey over the previous 4 years; then, suddenly, there was nothing. You cannot imagine what an honour and privilege it was to work with those children, and what it was like to be there as they discovered, and learned, and grew in confidence with their new-found ability to hear.
And the most difficult thing to come to terms with professionally was being prevented from writing up the case studies. David, Wendy, Joseph and Holly’s stories would have been important resources for the field. Pia’s story would have been turned into a book. She was right at the beginning of language development at the age of 6 when she suddenly began to hear with the cochlear implant. Her growth in language from that point would challenge the fundamental notion of there being a “critical period” for language development between birth and 6 years. I wanted to evaluate and guide Pia’s linguistic, phonologic, cognitive and discourse development as a postdoctoral research study, to keep it aligned as closely as possible to normal development. I had the perfect opportunity to compare and contrast her linguistic growth with that of my own one-year old daughter who was also at the same beginning stage of language. I think this was a lost opportunity, and I deeply regret not being able to write that book.
A colleague wrote a poignantly beautiful poem for me after these terrible events that encapsulates my raw feelings in the way only poetry can. It has provided me with consolation many times over the years when I most needed it.
As a postscript, the Australian-developed, multi-channel cochlear implant quickly became established as the most suitable implant for use with children, and it has now benefited thousands of children around the world.
I didn’t for one moment think this was going to be the end of my career, but that’s exactly what happened. As it turned out, I didn’t ever use my research qualifications or work in my profession again. It was not because I didn’t want to, or didn’t try, but I found to my absolute horror “the defamation” had gone way beyond the parents, and spread throughout the field in Australia and overseas. This meant that not only had I been wrongfully expelled from the work, but I was also wrongfully prevented from coming back into it. Who would hire someone who didn’t have a reference, and was whispered about for “misappropriating money” and “trying to stop the implant work”?
I was oblivious to what was being said about me, because I didn’t have any contact with anyone in the field for several years. I needed time to myself so I could come to terms with what had happened, and I was relieved I was finally able to be a mum and could spend time with my baby daughter. I found this new role to be a wonderful antidote to all the misery I had been put through. I also put the wheels in motion for the donor transplant operation with my sister. Her position had deteriorated so much we had to wait several months before she was strong enough to undergo the operation. But it was well worth the wait. The transplant was so successful her kidney started working straight away, and almost immediately you could see a change in her skin colour. She quickly returned to good health and lived a full life free from dialysis for the next 22 years. Her kidney finally failed in 2013 and I sadly lost my beloved sister, but she had had a good, long life until then.

My sister Laurel and me. She was my only sibling.
When my husband was in the final stages of completing his doctorate, and our daughter was nearing school age, I decided to put out feelers to get back into the cochlear implant field. We thought about going back to Canada, and I contacted the University of Western Ontario in London, Ontario because they had tried to headhunt me when I was just finalising work on my doctorate. I talked to the head of the department and told him about my 5 years’ experience with paediatric cochlear implants in Australia, and he was extremely interested in what I could offer. They were just about to start a children’s cochlear implant project at their university, and he was both surprised and pleased someone was available who had so much experience in the field. He said he would find out what he could do to set up a position, and get back to me. However, when he did, the whole tenor of the discussion was completely different. He told me he had called people in Australia and heard about “the trouble” with Professor Gibson. I asked him what he meant by this, and he said it was something about me “trying to stop the implant work”, and also something about me having been under investigation for “misappropriating money”. I couldn’t believe my ears because it was completely untrue.
I also applied for a position in the European division of Cochlear, with the same result. I didn’t even receive an acknowledgement of my application or get an interview and guessed that the defamation may have affected that organisation as well.
Then, last year, I inadvertently came across the transcript of a speech Professor Gibson had made at an Annual General Meeting entitled “The Long, Winding Road of the Cochlear Implant”. I was absolutely incensed to find the false and misleading things he had been saying about me in print. It is hard to believe someone who had already been sued for defamation was continuing in that vein thirty years later. I now, finally, want the truth about what happened to be known.

Left to Right: Pia Jeffrey, David Suutari, Joseph Silipo, Holly McDonell, Wendy McLean
The false and misleading statements about me were published in a book, a web journal and on a website. The specific statements and my responses are set out below.
“There were several deaf students at Chatswood Primary, and the small teaching team was given a cupboard outside a classroom in which to keep their apparatus. During the lunch hour, Maggie Loaney and Sylvia Romanik were allowed to use a classroom to program and teach the children. Peter Collins was the Minister for Health at the time. He visited Chatswood Primary and gave the team a grant to staff the house in nearby Anderson St that had been rented by Gibson, and to provide devices and follow-up services for 10 children a year.
Two major difficulties occurred. The senior teacher of the deaf decided to take control of the program and stop increasing the number of implants, and instead research in detail the children already implanted. After a power struggle, Gibson persuaded her to resign and take a non-clinical research role. About a month later he was summoned to Yu’s office for a discussion, as the teacher claimed that she had been wrongly dismissed and her job description had been changed illegally. Her claim was overruled after an inquiry and she resigned from the program.” (Pages 128-129)
This passage contains numerous misrepresentations and falsehoods. Specifically, sentence by sentence:
“There were several deaf students at Chatswood Primary, and the small teaching team was given a cupboard outside a classroom in which to keep their apparatus.”
This is incorrect because I wasn’t a teacher: I was a researcher, and Rosalie was a clinician who worked with the clinical program. We were not given a cupboard outside a classroom, we used a storeroom for the clinical work and for the apparatus. Please refer to the photos which show the small storeroom that I worked in.
“During the lunch hour, Maggie Loaney and Sylvia Romanik were allowed to use a classroom to program and teach the children.”
This falsely credits two teachers at Chatswood School with doing the work done by Rosalie and me. Maggie Loaney and Sylvia Romanik were teachers of the deaf at Chatswood School who were employed by the Education Department to run the OD (Opportunity Deaf Unit), and they had nothing to do with the programming and follow-up work. In fact, they strongly opposed one of their pupils, Pia Jeffrey, from getting an implant. Furthermore, they didn’t work in a classroom during their lunch hour. I worked full-time in the book storeroom, and Rosalie worked in the corridor.
“Peter Collins was the Minister for Health at the time. He visited Chatswood Primary and gave the team a grant to staff the house in nearby Anderson St that had been rented by Gibson, and to provide devices and follow-up services for 10 children a year.”
The Minister for Health did not just happen to visit Chatswood Primary School and give the team a grant. I wrote a letter to Peter Collins and he responded to my letter by allocating a large annual grant to the program. This grant was a direct result of me having taken this initiative.
“The senior teacher of the deaf decided to take control of the program and stop increasing the number of implants, and instead research in detail the children already implanted.”
This is false and misleading. First, I was a Senior Researcher, not a senior teacher; second, I wasn’t trying to stop increasing the number of implants. If you look at the quote from my letter to Professor Gibson in October 1988 I said:
“The current group of implantees is not getting a fair deal, and we certainly can’t accept more candidates until the problems are sorted out. However, I do not think the project should be limited by the resources that are currently available. We should be expanding those resources and building a strong program for the children in NSW.”
The paragraph in the book leaves out the rest of what I said about not being able to accept more candidates until all the problems were sorted out, and that we needed to build a strong program for the children in NSW.
“After a power struggle, Gibson persuaded her to resign and take a non-clinical research role.”
He didn’t persuade me to resign, he forced me to resign by making my position redundant. He didn’t persuade me to take a non-clinical research role because I was already a senior researcher. That was my job, but he stopped me from doing it.
“About a month later he was summoned to Yu’s office for a discussion, as the teacher claimed that she had been wrongly dismissed and her job description had been changed illegally.”
I didn’t claim my job description had been changed illegally. I merely wanted to carry out the work I was meant to be doing in my job description.
“Her claim was overruled after an inquiry and she resigned from the program.”
There was no inquiry about wrongful dismissal, and my claim was not overruled.
“Another crisis was that Gibson was accused of running a brothel in Anderson St. The neighbours had seen young women going to and fro from the house, and had jumped to the wrong conclusion.”
This is absurd. The house was right next door to a Catholic School, and generally men go in and out of brothels, not young women pushing strollers with toddlers and children in tow.
Who would mention something like this in a public forum in which they are recounting the history of the work, especially if it was their own mistake? Professor Gibson was the person who organised the rental arrangements and he is the one who failed to ensure he had the proper permits to use the house for a clinical program.
“There were two major downs. The first was there was an inquiry into the foundation, saying that there had been misappropriation by a teacher. That teacher was subsequently cleared”.
This is totally untrue. There wasn’t an inquiry into the Foundation about misappropriation by a teacher (supposedly me), who was later cleared.
“The neighbours in the house that we were renting claimed that the house was a brothel.”
This is absurd.
“... the neighbours took it into their heads that Gibson was running a brothel”.
Again, this is absurd.
“… a disgruntled colleague was behind claims he had misappropriated funds from the EAR (Ear And Related Research Foundation).”
This is incorrect. I didn’t claim Professor Gibson had misappropriated funds from the EAR Foundation. I went to the Pro Vice-Chancellor’s office about Professor Gibson’s unethical and unjust conduct and they referred matters to the Independent Commission Against Corruption (ICAC).
Writing this has been one of the hardest things I have ever had to do in my life. It has been extremely painful reliving the events that caused so much damage to me, to the children, and to the field.
I was so traumatised at the time I could only cope by avoiding having any contact with the field. I closed my ears to stories in the media about cochlear implants, and even took to driving on the ring road around Sydney whenever I headed north rather than pass through Chatswood where it all happened.
I kept on having a recurring nightmare of Professor Gibson deliberately driving full pelt into me in a car, and leaving me injured and dying on the road. All around, my colleagues and the parents just stood and watched, but no one came to offer any support.
I realised I couldn’t keep on living with such intense feelings of grief and loss and began to read widely about other people who had suffered traumatic, life-changing events. There were famous cases like Joern Utzon who was dismissed by the NSW Government from his role as architect of the Sydney Opera House. I fully understood why he didn’t ever want to come back to Sydney to see the finished work. I couldn’t begin to imagine the pain the brilliant cello player, Jacqueline du Pré, must have suffered when she was diagnosed in her late twenties with multiple sclerosis. And more recently, I’ve been inspired by Turia Pitt whose life was almost destroyed when she was terribly burnt in a bushfire. She has gone on to live a rich and fulfilling life despite her internal and external scars.
All these people and many others I read about helped me to move on. But the most significant benefit came from my own knowledge of what I had achieved in those 5 short years, despite the constant undermining and obstacles that were put in my path. I had the extraordinary experience of being at the forefront of a medical breakthrough that changed deafness forever. I was the person who actually discovered what children could do with cochlear implants, and I understood the ramifications and the impact these discoveries would have on the field. I was the person who broke the news to the field at the International Audiology Conference in Jerusalem in 1988. I was so overcome with the enormity of what I was about to announce when I started the presentation I couldn’t get any words out. I just showed the videotapes of the children and let them speak for themselves. Obviously, they had an enormous impact because professionals from around the world wrote to me afterwards requesting copies. They couldn’t wait for the scientific papers to be written, which actually didn’t ever happen.
As you can well imagine, I am deeply aggrieved that my pioneering work has been erased from the history of the field. The outstanding success of the children in the Pilot Program is largely due to my expertise, and the very positive media coverage we received had an enormous impact on the implant’s acceptance among the public and among professionals in the field. The tenor of opinion changed from scepticism to acclaim, and the rest is history.